

Introduction
Have you ever wondered whether a red light device can really change recovery outcomes? I pose that question because a simple scenario plays out in clinics every week: an athlete seeks faster recovery, a clinician recommends a device, and the patient signs up. The term red light bed appears in treatment notes, and yet outcomes vary widely. From a legalistic vantage — pursuant to consent frameworks and device classification criteria — the evidence base shows mixed effect sizes and varied reporting standards (some audits show modest functional gains). I cite these data not to confuse you, but to frame a precise query: which features truly matter when selecting a red light bed? This piece moves from that question into specific, actionable comparisons. Let’s dig into the finer faults and the real metrics that separate marketing from meaningful performance.
Unseen Flaws and User Frictions in light bed therapy
Why does it still feel inconsistent?
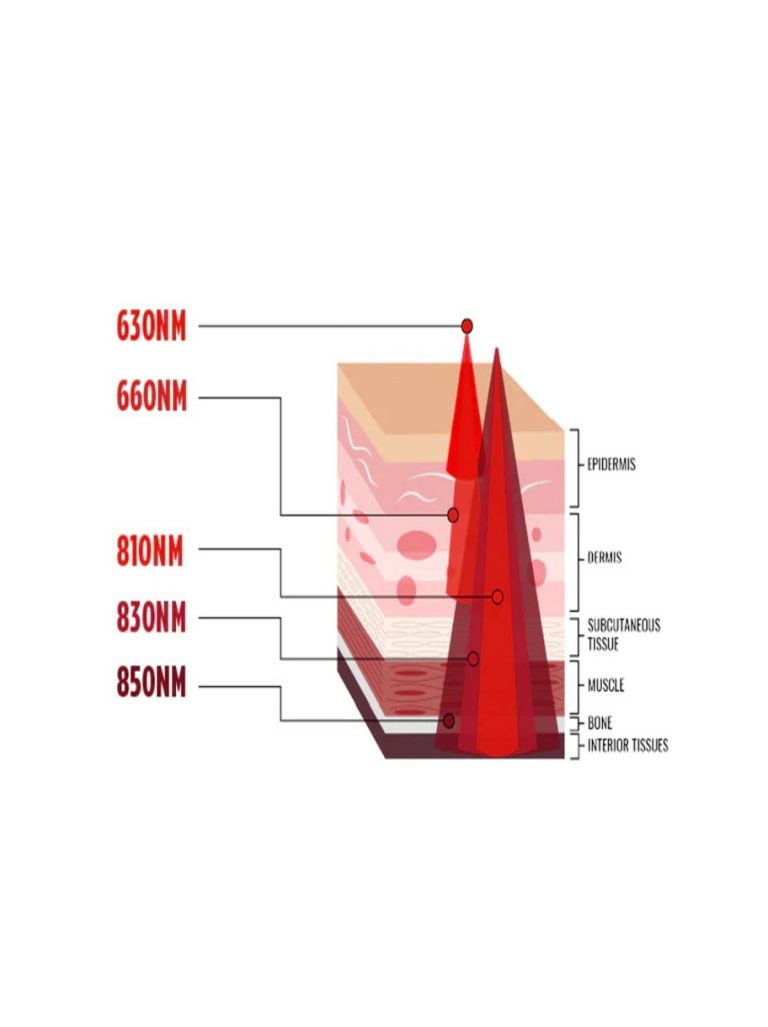
I start by breaking down the main technical culprits. Photobiomodulation depends on wavelength specificity and irradiance. When manufacturers blend LED arrays without consistent wavelength control, you see variable tissue responses. I’ve watched good clinics replace a unit because its output drifted — thermal management failed, and power converters skewed the spectrum. Those are hardware-level issues, not marketing spin. Look, it’s simpler than you think: inconsistent irradiance and poor wavelength fidelity yield uneven results.
On the user side, hidden pain points matter. Patients complain about session time, perceived heat, and unclear dosing. I’ve heard clinicians say the same thing: “We don’t trust the timer settings.” This distrust amplifies when maintenance is neglected. In practice, LED degradation, lack of calibrations, and weak cooling create a cascade — shorter lifespan, lower effective irradiance, and erratic photobiomodulation. Manufacturers often omit clear standards for clinical dosing. That gap forces clinicians to guess at treatment parameters, which harms reproducibility and patient trust. So yes, the flaws are technical and procedural, and they compound in real settings — funny how that works, right?
New Technology Principles and Practical Metrics for Choosing Devices
What’s Next — practical guidance?
Moving forward, I favor principles that marry robust engineering with clinical clarity. First, devices must specify wavelength bands and maintain wavelength specificity under load. Second, they should document sustained irradiance at the treatment surface (mW/cm²) across expected service life. Third, thermal management and reliable power converters are not optional; they protect LED arrays and preserve output. When I evaluate a device, I ask for calibration data, spectral plots, and longevity tests. These are not flashy, but they tell you whether a unit will perform in real clinics.

To be concrete, here are three metrics I recommend you use when comparing units. 1) Peak and sustained irradiance (measurements at standard distances). 2) Wavelength accuracy and narrowband reporting — not just “red” or “near-infrared.” 3) Thermal control and serviceability — can components be replaced; are power converters specified? Use these metrics to compare specs rather than marketing claims. I summarize: focus on reproducible output, engineering quality, and clear dosing guidance — you’ll save time and money. — and yes, I still prefer units that offer easy calibration access because clinicians actually use them. In closing, weigh these benchmarks carefully before purchase and consider manufacturer transparency as a core selection factor. Magique Power